
Individuals with intellectual and developmental disabilities, physical disabilities, behavioral health issues, cognitive impairments (e.g., Alzheimer’s or dementia), or serious mental illness often require long-term services and supports (LTSS).
LTSS includes an array of health and social services that help support these individuals with activities of daily living (ADLs), such as bathing, eating, and toileting, as well as instrumental activities of daily living (IADLs), such as medication management, budgeting, and transportation.
Individuals receive these services in a variety of settings, ranging from institutional facilities such as nursing homes or intermediate care facilities to congregate settings including assisted living centers and group homes to privately-owned homes or apartments.1
Over the last several years there has been an increased emphasis on home and community-based services (HCBS). States and the federal government have begun to work towards increasing access to HCBS to better manage care for consumers using LTSS and improve patient experience, quality of life, and health outcomes. HCBS has also been shown to be less costly than institutional care. It is generally accepted that three individuals can receive HCBS in the community for the cost of serving one person in an institutional facility.² This makes HCBS an appealing option for states as health care costs continue to rise.
As the primary payer and source of health care coverage for individuals with complex health conditions, Medicaid has a vested interest in designing programs that improve their quality of care while addressing the high cost associated with serving these individuals. Working in partnership with the Centers for Medicare and Medicaid Services (CMS), states are working towards designing programs that deliver high-quality systems of care for individuals with complex care needs.
Overview of the project and methodology
UnitedHealthcare Community and State (UnitedHealthcare), in partnership with its independent National Advisory Board, has undertaken a multi-year project to explore data and research to develop recommendations for benefit designs that better support people with disabilities of all ages and their caregivers. The goal is to achieve improved health and wellness while affording them greater flexibility and control over their lives.
The Board is composed of leading experts in aging and disability policy and practice, a UnitedHealthcare health plan member and a family caregiver of a child with special health care needs. The Board provided UnitedHealthcare with guidance and input to promote a better understanding of the needs of individuals with disabilities of all ages and their family caregivers, and of the programs and services that can best support them.
The project focused on creating benefit and program design recommendations that support the following four population groups:
- Individuals with Alzheimer’s or related dementias
- Individuals with physical disabilities
- Individuals with intellectual and developmental disabilities (I/DD)
- Individuals with behavioral and mental health conditions (including Serious Mental Illness and Substance Use Disorder (SUD))
The following conclusions and recommendations reflect the Board’s input and guidance. These recommendations are based on analysis of Medicaid waivers, including Section §1915(b), §1915(c), and §1115 demonstration waivers for all 50 states, Puerto Rico, and the District of Columbia, as well as state plans, where readily available. Additional information from published literature and other reports, along with the team’s waiver knowledge, were also used to support this initiative.
The Board’s recommendations aim to:
- Be person-centered;
- Support a holistic view of sustainable long-term health and well-being rooted in communities; and
- Serve individuals in a culturally-competent manner
UnitedHealthcare is committed to leveraging the research and recommendations associated with this project to support individuals with chronic and/or disabling health conditions and their caregivers.
Medicaid state plans and waivers
While federal regulations set the requirements for state-operated Medicaid programs and mandates coverage of some populations and certain benefits, many coverage and benefit decisions are up to the individual states. For example, states decide who is eligible beyond mandated populations, which optional services will be covered, and what the payments for services will be. Figure 1 compares the mandatory benefits that states are required to cover per federal regulations and the optional benefits that are at states’ discretion. Each state is required to submit a comprehensive document to CMS outlining the scope of its Medicaid program in its State Plan.
Figure 1: State Plan Benefits: Mandatory and Optional 3

State plan services and eligibility options are entitlements, and the state plan prohibits states from establishing annual benefit maximums for an individual, setting enrollment limits, or maintaining waiting lists.
However, states that want additional flexibility to design different benefit packages for specific populations, to restrict individuals to certain providers, or to extend coverage to groups beyond what is defined in Medicaid law can apply for a waiver of the federal Medicaid statute.
Some of the most common waivers that states leverage include the following:
- §1115 demonstration waivers
- §1915(b) waivers
- §1915(c) waivers
Figure 2 provides details on the differences between the state plan and the most commonly used Medicaid waivers.
Figure 2: Comparison of State Plan and Various Medicaid Waivers 4

Waivers can help states accomplish a number of different objectives, including:
- Providing benefits that are targeted to specific groups of individuals based upon diagnosis, disability, and/or geographic regions;
- Expanding eligibility to groups not traditionally covered by Medicaid;
- Experimenting with new service delivery methods or benefit design; or
- Enrolling individuals into managed care plans
States leverage waiver flexibility to customize their Medicaid programs to meet their unique needs. This flexibility allows states to make decisions about their specific program design, inclusive of eligibility, delivery system, premiums and cost sharing, and optional benefits. For LTSS, many states have designed waivers that allow them to provide services to individuals at home or in the community instead of in institutional settings, allowing individuals to remain as independent as possible.
All 50 states use some type of waiver authority to provide HCBS benefits to individuals, and in some instances, their caregivers. However, the number, type, and scope of Medicaid waivers vary considerably across states. Most states use §1915(c) waivers to meet the needs of people in need of LTSS in their home or community instead of an institutional setting or long-term care facility. Some states also leverage §1915(c) waivers to provide respite care, training, and family counseling. In waiver programs, many states permit individuals to hire family members as caregivers directly.
The majority of states currently elect to provide HCBS benefits through §1915(c) waivers. An alternative to using §1915(c) waivers to provide HCBS benefits is through §1115 demonstrations. Rhode Island and Arizona are among the states that utilize this flexibility.
Designing benefits to support individuals with complex needs
HCBS benefits should provide maximum flexibility to enable persons with complex health needs to live with dignity and independence in the community by expanding, strengthening, and integrating systems of community-based long-term supports that are person-centered.
The majority of the LTSS that aide individuals with functional limitations should be available to all waiver recipients, regardless of diagnosis. States can also choose to target benefits to specific populations based on functional diagnosis and in accordance with their person-centered plan. This would allow states to limit access to those who actually need these supports through state-defined medical necessity criteria. For example, individuals with physical disabilities may not need benefits such as assertive community treatment (ACT) or dialectic behavioral services; whereas, individuals with serious mental illness are likely to benefit from these services.
Benefit designs should reflect that individuals are unique and come from a variety of backgrounds. Each state has a different demographic set of ethnic, racial, religious, geographic, or social minority groups—many of whom experience unequal access to and outcomes from HCBS systems. The decision-making authorities in each state are trusted to develop and exercise their cultural competency when creating waiver systems. Effective cultural competency goes beyond merely identifying the needs and values of individuals with diverse cultural backgrounds; plan designers must treat these differences respectfully and actively work to address these differences in the fundamental structures of the waiver systems they create.
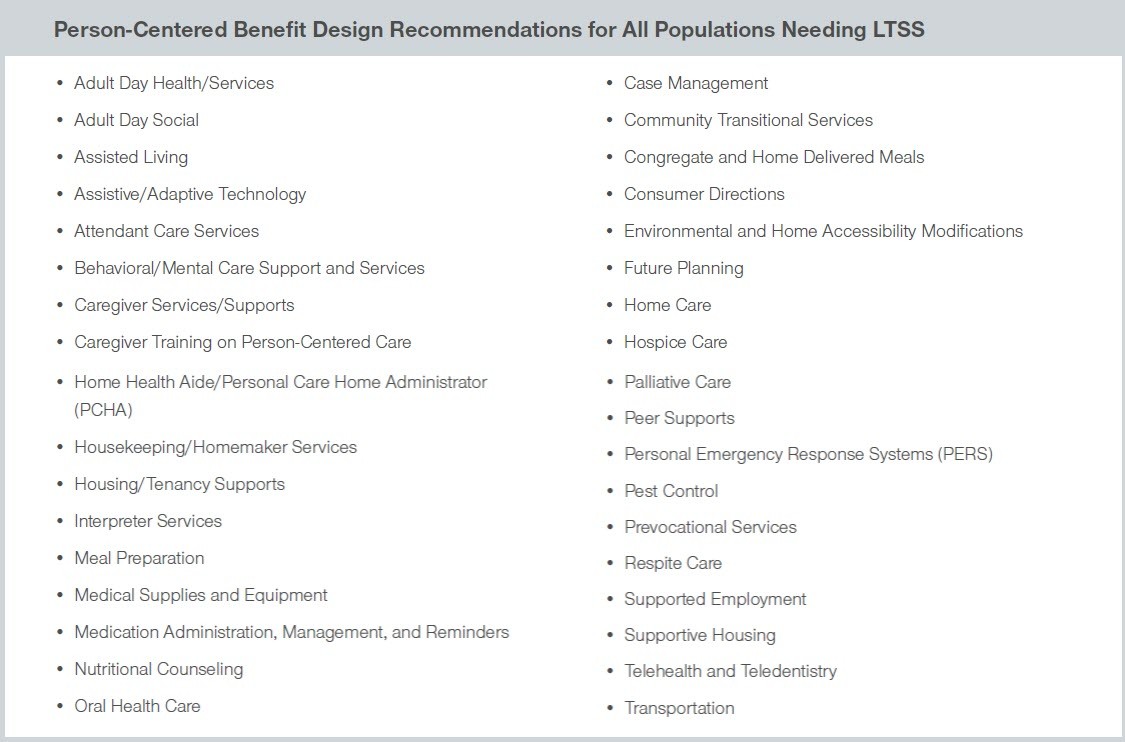
UnitedHealthcare and its Board recommend that states make available the benefits and services shown in Figure 3 to all individuals in need of LTSS. States should provide these benefits to individuals based on their needs and desires and in alignment with their person-centered care plan (and not solely on diagnosis).
Figure 3: Person-Centered Benefit Design Recommendations for All Populations Needing LTSS
In addition to the comprehensive benefits to be offered to individuals who are in need of LTSS, UnitedHealthcare and the Board recommend that states offer additional benefits to individuals with certain functional diagnoses and in accordance with their care plan, which are detailed in Figure 4.
Figure 4: Additional Benefit Design Recommendations for Individuals with Intellectual Disabilities and Developmental Disabilities, Behavioral and Mental Health Conditions, and Alzheimer’s or Related Dementias

The Appendix provided at the end of this document includes general definitions of all of the benefits listed in Figures 3 and 4.
Leveraging Medicaid waivers to support state priorities
Administrative requirements for Medicaid waivers
While Medicaid waivers provide states with additional flexibility to design programs that differ from what is required by federal rules, the administrative requirements that accompany applying for and implementing these waivers are extensive. States seeking to leverage waiver flexibility must develop waiver requests and submit them to CMS. CMS requires significant stakeholder engagement on all waivers. For §1115 demonstration waivers, states must meet certain transparency requirements before submission, which usually involves holding a public comment period. States must also obtain public input during the development of §1915(b) or §1915(c) waivers and make the waiver draft publicly available prior to submission.
After the prerequisites for the waiver request are met, the state must then submit the request to CMS. The approval process varies by the type of waiver. While CMS has at least 90 days to approve §1915(b) and §1915(c) waivers, CMS usually takes much longer to review and approve §1115 demonstration waivers. As part of the §1115 demonstration waiver approval process, CMS and states often engage in prolonged negotiations, during which time the waiver request may undergo several changes. After a waiver is approved, states must evaluate their program and submit frequent (quarterly and annual) reports to CMS.
States that operate multiple waivers must undertake additional administrative responsibilities. As detailed above, each specific waiver requires its own application, must be renewed individually, and has separate and distinct reporting requirements, as mandated by CMS. States must also oversee multiple contracts and contractors, maintain separate systems and processes, manage multiple waiting lists and program budgets, and administer multiple quality programs, among other administrative tasks. Additionally, in many states, each waiver is managed by a different statewide administrative entity, which further complicates program administration.
Achieving administrative effectiveness
Despite the administrative complications associated with operating multiple HCBS waiver programs, most states still use multiple waivers to provide HCBS to individuals in need of LTSS.
Federal authority, however, provides states with the flexibility to serve individuals of different target groups under one waiver.⁵ On January 16, 2014, CMS published a final rule (42 CFR 441.301 (b)(6)) that permits states to combine target groups within one waiver, removing a barrier for states that wish to design a waiver that meets the needs of more than one target population. The provision of the rule related to target groups provides an option to states to design services across populations, which may lead to improved integration and administrative efficiencies in state Medicaid agencies.
To operate under this rule, a waiver must be limited to one or more of the following target groups or any subgroup thereof that the state may define:
- Aged or disabled, or both
- Individuals with Intellectual or Developmental Disabilities, or both
- Mentally ill
Through this guidance, CMS was attempting to create some standardization on key program elements related to policy objectives that are of importance to stakeholders, providers, and policymakers. The guidance was also intended to provide states with the flexibility needed to evolve their programs. Prior to this regulation, states were required to develop separate §1915(b) and §1915(c) waivers to serve more than one of the specified target groups; this resulted in states simultaneously operating numerous waivers, for example ranging anywhere from one to 11 §1915(c) waivers in a single state.
Despite this flexibility, many states still administer several waivers to provide services to a variety of populations. In addition to the administrative burden that administering multiple waivers creates, it also causes confusion for individuals in need of services, and often results in misalignment of services to individual needs.
Recommendations
Streamline and consolidate existing waivers
States should look for opportunities to streamline and consolidate their existing waivers to create program efficiency by decreasing the administrative complexity inherent when operating multiple waivers.
The current Medicaid HCBS system creates confusion for individuals in need of services. Individuals seeking services have to navigate the program’s complexities, which include different benefits and eligibility requirements, in order to determine which program best meets their needs. Creating a system that is easy to navigate facilitates the ability for individuals to get the services and information they need and improves consumer experience.
For example, one benefit package may include personal care for people with physical limitations, while another benefit package may provide specialty behavioral health services. If different services are offered through distinct programs, people with multiple needs will have to choose which services to pursue and which to forgo.⁶ There are many benefits to streamlining Medicaid HCBS programs into a single waiver, including:
- Allows states to serve individuals of different target groups who live together (e.g. an individual with an intellectual disability and his/her aging parent) seamlessly
- Reduces administrative costs and frees up funds for the provision of services with no bottom line impact to the overall state budget
- Recognizes that individuals’ needs may make them eligible under multiple eligibility groups and offers an array of services to meet a wide arrange of needs, regardless of diagnostic category
- Encourages person-centered approaches to care by enabling alignment of services to specific needs rather than aligning to specific waiver design
- Encourages administrative efficiencies for states that offer the same benefits to multiple target groups using multiple waivers
- Decreases administrative complexity for states by moving away from a piecemeal approach, as they will not have to combine multiple authorities, administer different sets of eligibility rules, and oversee distinct quality measures
Ensure program design simultaneously improves care and contains costs
While there are several advantages for states opting to consolidate their waivers, states must also ensure that their program design recommendations simultaneously improve care and contain costs. Federal regulation requires that states must demonstrate cost neutrality in their waivers, while emphasizing preventative care and keeping people healthy. Cost neutrality requires that spending on waiver services cannot be greater than they would be in the absence of the waiver. States considering consolidating multiple HCBS waivers must carefully weigh cost neutrality requirements and long-term program savings against the administrative efficiencies achieved through waiver consolidation. When designing programs, states should make investments in quality care upfront in order to ensure the cost-effective use of resources.
Strengthen self-care supports for caregivers
Caregivers face a number of challenges. It can often be difficult for them to find time for themselves, potentially leading to fatigue, distress, or health issues of their own. Existing Medicaid authorities can be used to strengthen caregiver supports, especially §1915(c) waivers. Waivers allow states to provide support to caregivers including respite care, training and educational opportunities, and counseling. Ensuring caregivers are supported will positively affect the individuals they are caring for. Therefore, assuring that caregivers are aware of these resources is critical.
Guarantee programs are in alignment with federal guidelines
As states consider consolidating or streamlining their waivers to customize their programs and provide a defined set of HCBS to targeted populations, states must ensure the following:
- Each individual within the waiver, regardless of target group, must have equal access to the services necessary to meet their unique needs as indicated in the person-centered plan; and
- States may not limit services based on an individual’s target group; for instance, states cannot mandate that the Personal Emergency Response Systems (PERS) benefit is only for older adults or that individuals with I/DD can only access habilitation services.
Conclusion
As states continue to navigate complex political and budgetary environments, they along with CMS continue to look for ways to improve the availability and delivery of LTSS. It is imperative that the federal government, states, stakeholders, beneficiaries, and insurers work together to design programs and provide benefits that are most appropriate for individuals with complex health needs.
UnitedHealthcare and its National Advisory Board are dedicated to ensuring that individuals of all ages with intellectual and developmental disabilities, physical disabilities, behavioral health diagnoses, cognitive impairments, or serious mental illness have access to the services they need to live healthier lives in the community as well as greater flexibility and control over their own lives.
Sources
- C. Dobson, S. Gibbs, A. Mosey, and L. Smith. Demonstrating the Value of Medicaid MLTSS Programs. National Association of States United for Aging and Disabilities (NASUAD) MLTSS Institute. May 2017 Opens in a new window
- “Providing More Long Term Support and Services at Home: Why It’s Critical for Health Reform.” Fact Sheet. AARP Public Policy Institute. 2009
- “Mandatory & Optional Medicaid Benefits,” Medicaid.gov, Centers for Medicare & Medicaid Services Opens in a new window
- Adapted from https://www.macpac.gov/topics/waivers/ and Information from Medicaid.gov
- A provision of the 2014 1915(c) HCBS Final Regulation permits states to serve multiple target groups under one 1915(c) waiver.
- Streamlining Medicaid Home and Community-Based Services: Key Policy Questions Opens in a new window
- Peebles, Victoria and Alex Bohl. “The HCBS Taxonomy: A New Language for Classifying Home and Community Based Services.” Centers for Medicare and Medicaid Services Medicaid Policy Brief. Brief 19. August 2013. Opens in a new window
National Advisory Board’s Recommended Benefits to Support Individuals with Complex Health Needs In Agreeance with 2013 Taxonomy7
- Adult Day Health/Services: Community-based group programs designed to meet the needs of adults with disabilities through individual plans of care. Services can include health education, self-care training, therapeutic activities, and health screening. Intensity of services received depends on the needs of the individual.
- Adult Day Social: Provides interaction with other individuals utilizing services through planned activities appropriate to an individual’s specific condition.
- Assertive Community Treatment (ACT): An evidenced-based practice that offers treatment, rehabilitation, and support services using a person-centered, recovery-based approach to individuals that have been diagnosed with a severe and persistent mental illness. The goal is to assist these individuals to achieve their personally meaningful goals and life roles. Services can include assertive outreach, mental health treatment, health, vocational, integrated dual disorder treatment, family education, wellness skills, community linkages, and peer support.
- Assisted Living: Housing for older adults or individuals living with disabilities that provides custodial care including nursing care, housekeeping, meals, medication management, and a number of other services. Individuals can live independently, but receive assistance for services they have difficulty with. Commonly used alternative language: Adult family homes, adult foster care, adult living facilities, board and care, domiciliary care, eldercare facilities, group homes, memory care facilities, personal care homes, residential care facilities, senior living residences, sheltered housing, supportive living.
- Assistive/Adaptive Technology: Includes devices, pieces of equipment, or products that are modified or customized and are used to increase, maintain, or improve functional capabilities of individuals with disabilities. Assistive technology services also include any service that directly assists a disabled individual in the selection, acquisition, or use of an assistive technology device, including evaluation of need, acquisition, selection, design, fitting, customization, adaptation, and application.
- Attendant Care Services: Services provided to assist residents with activities of daily living such as eating, bathing, dressing, personal hygiene, and other activities of daily living. Services may include assistance with preparation of meals, but not the cost of the meals themselves. When specified in the plan of care, this service may also include such housekeeping chores as bed-making, dusting, and vacuuming, which are essential to the health and welfare of the recipient. Attendants may be the participant’s family member, except the participant’s spouse. Commonly used alternative language: Personal care services, personal assistance services, personal attendant care.
- Behavioral/Mental Care Support and Services: Training, supervision, or assistance in appropriate expression of emotions and desires, compliance, assertiveness, acquisition of socially appropriate behaviors, and the reduction of inappropriate behaviors.
- Caregiver Services/Supports: Supportive services provided for caregivers of individuals needing LTSS services. Caregivers are individuals providing unpaid assistance to individuals receiving LTSS. Supports can be emotional, such as access to helplines, or task related. Common caregiver supports provided through §1915(c) waivers include but are not limited to respite care, training, and family counseling.
- Caregiver Training on Person-Centered Care: Training for individuals who provide care and support for individuals of all ages with intellectual and developmental disabilities, physical disabilities, behavioral health diagnoses, cognitive, or serious mental illness that focuses on the individuals needing care. Training helps familiarize caregivers with different types of situations they may face.
- Case Management: Case management is a system under which a designated person or organization is responsible for locating, coordinating, and monitoring a group of services. A case manager is responsible for outreach, intake, and referral, diagnosis and evaluation, assessment, care plan development, and implementing and tracking services to an individual. The case manager is also responsible for authorization of waiver and non- waiver services included in the recipient’s care plan, terminations and transfers and maintenance of recipient records. Commonly used alternative language: Service coordination
- Cognitive Behavioral Therapy (CBT): A common type of psychotherapy that focuses on investigating the relationships between the thoughts, feelings, and behaviors of an individual. It is the goal of CBT to identify what is causing self-destructive behaviors and beliefs through identifying unhealthy patterns of thought. Individuals can then work to restructure thought patterns and work towards developing healthier behaviors and beliefs.
- Community Transitional Services: Community Transitional Services include reasonable, one-time set-up expenses for individuals who make the transition from an institution to their own home in the community and will not be reimbursable on any subsequent move.
- Congregate and Home Delivered Meals: Meals served in group settings, designed to meet the needs of specific individuals utilizing services.
- Consumer Directions: Also referred to as self-directed services. Service recipients have decision-making authority and manage their services with available supports. This promotes personal choice and empowerment for individuals with disabilities.
- Coordinated Specialty Care (CSC)- RAISE : A recovery-oriented treatment program for people with first episode psychosis (FEP). CSC promotes shared decision-making and uses a team of specialists who work with individuals to create a personal treatment plan. The individual and care team work together to make treatment decisions and attempt to involve family members as much as possible. The goal is to link the individual with a CSC team as soon as possible after psychotic symptoms begin.
- Day Supports: See definition for adult day health, but with added focus on the specific needs of an individual’s disability.
- Dialectic Behavioral Therapy (DBT): A common type of psychotherapy primarily focused on individuals with borderline personality disorder (BPD). DBT is based on cognitive behavioral therapy (CBT), but places a larger emphasis on the validation and acceptance of uncomfortable thoughts, feelings, and behaviors and seeks to find a balance between acceptance and change.
- Environmental and Home Accessibility Adaptations: Physical adaptations to the home, required by the individual’s plan of care, that are necessary to ensure the health, welfare, and safety of the individual or enable the individual to function with greater independence in the home. Providing environmental adaptations allows individuals to remain in their home environment as opposed to entering institutional care. The cost savings of avoiding institutional care makes these services financially sensible. Such adaptations may include the installation of ramps and grab-bars and/or the widening of doorways in order to accommodate the medical equipment and supplies necessary for the welfare of the individual.
- Future Planning: Planning for individuals with cognitive disabilities, including Alzheimer’s and dementia, to ensure their wishes are met. Planning can include financial, legal, and those related to end-of-life care and support. Planning should begin as soon as a diagnosis is made to ensure that the affected individual is able to participate to the fullest extent possible.
- Home Care: This service allows individuals to receive care in the home or community, as opposed to institutional facilities.
- Home Health Aide/Personal Care Home Administrator (PCHA): Support patients with a number of custodial needs and monitoring. They provide basic services including administering medications, changing bandages, general grooming, and checking vital signs. Services provided are similar to those in assisted living, but occur within an individual’s residence.
- Hospice Care: A specialized type of care for individuals with life limiting illness. It addresses the individual’s physical, emotional, social, and spiritual needs. Care is used when curative treatments are no longer an option and the individual is expected to live six months or less.
- Housekeeping/Homemaker Services: Homemaker services are general household activities that include meal preparation, food shopping, bill paying, routine cleaning, and personal services. Provided by a trained homemaker when the individual regularly responsible for these activities is temporarily absent or is unable to manage the home and care for him/herself. Commonly used alternative language: Companion services, Attendant services,
- Housing/Tenancy Supports: Services that help individuals enter into and remain in stable housing situations including but not limited to assistance to apply for housing, landlord supports, and skills training.
- Integrated Dual Disorder Treatment (IDDT): An evidence-based practice that improves quality of life for people with co-occurring severe mental illness and substance use disorders by combining substance abuse services with mental health services. It helps people address both disorders at the same time, in the same service organization, and by the same team of treatment providers.
- Interpreter Services: Language services provided to individuals with Limited English Proficiency (LEP) or individuals with hearing impairments utilizing American Sign Language (ASL). Any provider receiving federal funding from CMS is required to provide these services for individuals with LEP.
- Meal Preparation: Nutrition services provided to individuals living at home. Prepared meals are provided to individuals unable to cook for themselves or without caregiver support.
- Medical Supplies and Equipment: Includes devices, controls, or appliances specified in the plan of care, which enable recipients to increase their ability to perform activities of daily living or to perceive, control, or communicate with the environment in which they live. Included items are those necessary for life support, ancillary supplies, and equipment necessary to the proper functioning of such items, and durable and non-durable medical equipment not available under the Medicaid State Plan.
- Medication Administration, Management, and Reminders: A variety of services available to help individuals take their medications in the correct quantities, at the correct times, and to avoid any potential drug interactions. Services can range from traditional pillboxes to electronic reminders and alerts if any issues arise.
- Mobile Response Teams: Mental health professionals that provide services to individuals outside of traditional clinical settings, including at home. Mobile teams are often used in emergencies or during mental health crises.
- Nutritional Counseling: An individually designed service which provides an assessment of the participant’s nutritional needs and food patterns, and the planning for the provision of food and drink appropriate for the participant’s conditions, or the provision of nutrition education and counseling to meet normal and therapeutic needs.
- Oral Health Care: Medical care focusing on the mouth, teeth, and gums.
- Palliative Care: Care provided to individuals with conditions with no expectation of a cure or remission, with the overall aim of relieving pain and controlling symptoms. Palliative care focuses on the whole person, targeting both physical and emotional comfort. It is often provided in conjunction with other medical treatments and hospice care.
- Peer Supports: A type of service that engages individuals with disabilities living independently in the community to provide experience, knowledge, and expertise to assist other individuals in recovery and resiliency to allow them to become more independent in their communities. The specific provision of this service depends on the agency or organization providing it.
- Personal Emergency Response System (PERS): PERS is an electronic device that enables certain high-risk individuals to secure help in the event of an emergency. The recipient may also wear a portable “help” button to allow for mobility. The system is connected to an individual’s phone and programmed to signal a response center once a “help” button is activated. PERS must be provided by trained professionals.
- Pest Control: Aids in maintaining an environment free of insects such as bed bugs, roaches, and other potential disease carriers to enhance safety, sanitation, and cleanliness of the participant’s home and/or residence.
- Prevocational Services: Readiness activities and teaching aimed at preparing individuals with disabilities for employment or other community activities. Includes the teaching of concepts such as compliance, task
- completion, attention, problem solving, and safety. Prevocational services are provided to persons not expected to be able to join the general workforce within one year.
- Respite Care: This service provides temporary relief to primary caregivers from the ongoing responsibility of caring for individuals. Respite can be informal, through the utilization of a family or friend, or formal through providing trained caregivers to attend to the short-term needs of an individual. Respite care may be provided in the recipient’s home, place of residence, or an approved facility.
- Supported Employment: This service provides supports to individuals in achieving employment within the community or through self-employment. Services can include career planning, employment assistance, and job-coaching. Supports should target the goals of the individual, not their readiness or ability.
- Supportive Housing: Assists individuals to obtain and maintain affordable housing through housing case management and tenancy supports. Services can allow the transition from institutional settings to the community.
- Telehealth and Teledentistry: The provision of health care remotely by means of telecommunications technology.
- Transportation: The provision of transportation to enable individuals to gain access to a variety of services including medical services, non-medical community services, resources/destinations, or places of employment. This resource allows individuals to maintain or improve their mobility within the community, increase independence and community participation, and prevent institutionalization.
